Is there a specific test that Diagnoses IBS?
NO.
Until now, we know little about what causes IBS.
So, until now, there has been no specific blood or stool test to diagnose IBS.
IBS is classified as a “functional disorder.”
A “functional disorder” means that we could not identify a cause of IBS using available tests (blood, stool, imaging techniques, and endoscopy).
However,
In 2015, Dr. Mark Pimentel, MD, first introduced a blood test for IBS-D diarrhea that helped differentiate between IBS-Diarrhea and IBD (inflammatory bowel diseases like Crohn’s and Ulcerative Colitis).
But the test is only valid for IBS diarrhea and not specific for all types of IBS.
Additionally, it has a low sensitivity for detecting IBS diarrhea (44%) (reference), so it is not used in daily practice by doctors.
How is IBS diagnosed using Rome criteria?
In May 2016, Rome IV criteria were reintroduced as symptom-based criteria to diagnose IBS.
It is widely used and still the most accepted way of diagnosing IBS.

A simplified way to diagnose yourself with Rome criteria:
| criterion | explanation |
| 1- Onset: 6 months | your abdominal pain started to occur for six months or longer. If you started experiencing abdominal pain in fewer than six months, it is probably not IBS. |
| 2- frequency of symptoms: | At least one day per week for the last three months |
| 3- main symptom: abdominal pain | Abdominal pain: occurs anywhere in your abdomen |
| 4- abdominal pain must be associated with at least 2 of the following: | 1- change in stool frequency: With the onset of the abdominal pain, there may be diarrhea or constipation or alternating diarrhea and constipation. |
| 2- the pain is associated with defecation: which means that abdominal pain is relieved by defecation. Or increased during defecation. | |
| 3- the pain is associated with a change in stool form (appearance): stools become hard or soft (even without diarrhea or constipation. |
You Can Diagnose Yourself By Asking Yourself These Questions:
1- when you first experienced abdominal pain?
If less than six months: Rome IV criteria not applicable (symptom onset should be six months or longer.
If more than six months: proceed to the second question.
2- Can you stay for more than a week in the last three months without abdominal pain?
If Yes: Rome IV criteria are not applicable (abdominal pain frequency should occur at least once a week in the last three months.
If No: Proceed to the next question.
3- With the onset of pain, do you experience diarrhea or constipation? (change in stool frequency).
4- Does the stool become harder or soft with the onset of pain? (change in stool form)
5- does the abdominal pain relieved or increased during or after defecation?
For questions 3, 4, and 5, the answer must be “yes” for at least 2 of these three questions for diagnosing IBS.
How are IBS Subytypes Diagnosed?
Before we diagnose you with any IBS subtypes, we have to:
- First, stop any IBS drugs that modify your IBS symptoms.
- Exclude any other drugs that cause diarrhea or constipation.
Examples of drugs causing diarrhea:
- Nonsteroidal Anti-inflammatory drugs: Ibuprofen and Diclofenac.
- Proton pump Inhibitors: Omeprazole and Esomeprazole (Nexium).
- Digoxin (Lanoxin): a drug that is used in certain patients with heart disease
Examples of drugs causing constipation:
- Iron preparations: used in patients with iron deficiency anemia.
- Norvasc: a drug used for hypertension and certain heart diseases.
- Some antiparkinson, anti-depressant drugs.
- Ideally, I inform my patient to keep a diary of abdominal pain and stool form for two weeks
- We usually use the “Bristol Stool Form Scale” to evaluate the type of IBS.
- Type 1 & 2 Bristol stools are the hardest ( type 1 is separate hard lumps that are hard to pass, and type 2 is lumpy sausage-shaped that is hard to pass).
- Type 6 & 7 are the loosest (type 6 is Fluffy pieces with ragged edges; mushy, and type 7 is watery.)
How Are IBS diarrhea, Constipation, And Mixed diagnosed? (DIY, step-by-step)
Here are the steps you can take to diagnose yourself with IBS diarrhea.
1- learn about the Bristol Stool Form Scale (BSFS): as we mentioned above.
2- stop IBS medications or any other medication for two weeks.
3- keep a diary of the days you have abdominal pain (IBS pain).
4- Record the number of your bowel habits (number of stool motions) only on the days with abdominal pain.
5- for every stool motion, also record the bristol stool form scale (1 to 7)
6- calculate the percentage of stool motions with bristol stool forms 6 and 7 of the total stool motions.
7- calculate the percentage of the number of stool motions with bristol stool form 1 & 2 of the total number of stool motions.
8- IBS-diarrhea is diagnosed when you have more than 25% of your stool motions with diarrhea (BSFS 6&7), provided that your constipation stool motions (BSFS 1&2) are less than 25% of the total number of stool motions.
Example: if you kept a diary of your abdominal pain and BSFS for two weeks:
- Out of the two weeks, there were only nine days with abdominal pain; during these nine days, you had 24 motions stool motions in total (exclude stool motions on days you don’t have abdominal pain)
- From the 24 stool motions, you have nine motions with diarrhea (BSFS 6 or 7).
- And only one stool motion with constipation (BSFS 1 or 2).
- then calculate the percentage of motions with diarrhea = (9/24) X100 = 37.5% (more than 25).
- And calculate the percentage of motions with constipation (2/24) X100 = 8.3% (Less than 25%)
- So this is diarrhea-predominant IBS.
9- IBS-constipation is diagnosed when the opposite occurs (more than 25% are constipation and less than 25% are diarrhea).
10- IBS-Mixed is diagnosed when constipation and diarrhea are more than 25% of the total stool motions.
11- IBS-Unclassified is diagnosed when constipation and diarrhea-predominant motions are less than 25% of the total stool motions during days of abdominal pain.
Can Rome’s Criteria Be wrong?
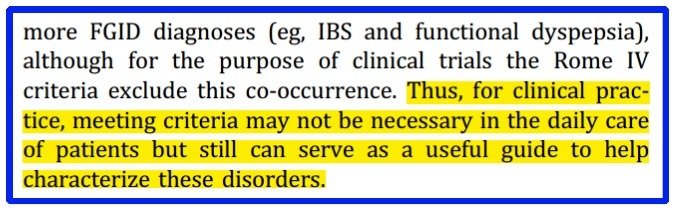
The Rome criteria are developed mainly To “HELP” in diagnosing IBS. It is not the ultimate truth about the presence of IBS.
We -doctors- still judge every patient on an individual basis, and this is according to the Rome criteria itself. (see screenshot below from Rome criteria publication):
And here is why:
1 when we (doctors) develop symptom-based criteria for a disease diagnosis, we don’t fully understand this disease.
2- the symptom Based criteria in Rome IV (abdominal pain and its association with mealtime, change in stool form or frequency) occur in a wide variety of other diseases inside your gut like:
- Food sensitivities (diet intolerance)
- Inflammatory bowel diseases.
- Bile acid malabsorption.
- Celiac disease
- Colon cancer
- Post-infectious malabsorption (tropical sprue)
- SIBO (small intestinal bacterial overgrowth).
- Gastritis.
- Cholecystitis
- GERD (Gastro-Esophageal Reflux Disease).
Although these above-listed diseases have more reliable methods of diagnosis, they always get confused with IBS.
I advise you always to ask your doctor about your symptoms if you’re not sure about your symptoms.
3- New onset IBS (less than six months) is not included in Rome criteria.
4- Rome criteria are not applied alone; we (doctors) may need to ask some other questions or do some tests to confirm a diagnosis of IBS.
These questions and tests are directed mainly to exclude other diseases resembling IBS.
The tests and questions are different for every patient according to their age, sex, existing diseases, and specific complaints.
So, Rome Criteria are a great tool to “Approach” the truth, but it is not the truth about IBS.”
When we suspect that you may don’t have IBS? (Red Flags):
1- A family history of colorectal cancer:
If one of your family members has a history of colorectal cancer, you should take your gut symptoms more seriously.
Colon cancer symptoms may resemble IBS. You must consult your doctor about any gut pain, abnormal stool, or blood in the stool.
In this article, I’ve thoroughly discussed how to know the difference between IBS and colon cancer.
2- A passage of blood with stool:
Blood in stool is not a symptom of IBS, the commonest cause of bloody stool with IBS is piles and anal fissures, but also inflammatory bowel diseases like ulcerative colitis or colon cancer may be the cause of your blood in the stool.
My advice to you: first, plan an appointment with your doctor; second, you can read this article that enlists all the causes of blood in stool with IBS.
3- weight loss:
Weight loss usually doesn’t occur with IBS. The presence of significant weight loss together with abdominal pain is common with conditions like:
- Inflammatory Bowel diseases (Crohn’s and ulcerative colitis)
- Colon cancer (or any other cancer).
- Malabsorption syndrome.
- Some rare infections like abdominal tuberculosis.
- Or it could be simply due to dietary habits (if you are eating less)
The bottom line is that you must define the cause of weight loss with your doctor.
4- Anemia
Anemia may indicate blood loss (even unnoticed) or other diseases like celiac disease. Discuss the issue with your doctor.
How doctors diagnose you with IBS (the complete steps I take):
The complete process of diagnosing IBS includes the following:
1- taking accurate history and planning follow-up visits to establish the diagnosis.
2- perform a thorough clinical examination.
3- perform limited tests in selected patients (including colonoscopy).
1- Take An Accurate History, If Needed, and Planning Follow-up Visits To Establish The Diagnosis.
- First, I ask about the history of abdominal pain and associated symptoms (applying Rome IV criteria).
- I ask for alarm features (family history of colon cancer, family history of IBD, blood in the stool, anemia, weight loss, late onset of the IBS after the age of 50)
- I Take detailed dietary history, especially the intake of dairy products.
- I ask about any drug history, especially those causing constipation, diarrhea, or gut upset.
- I may need a follow-up visit if the diagnosis is unclear (especially for detecting the subtype of IBS).
2- Perform a thorough clinical examination.
- We usually don’t find great signs of IBS, but the main aim is to exclude other diseases.
- In patients with IBS Constipation, we may need to perform a digital rectal examination to exclude hemorrhoids and fissures.
3- Perform limited tests in selected patients.
When we perform tests for IBS:
- Have one or more of the alarm features
- Testing for infectious diarrhea, IBS, and celiac disease is performed for patients with IBS diarrhea.
- We may consider a colonoscopy if you are older than 50 or have blood in your stool or weight loss.
- If you have severe constipation, we may need to perform abdominal radiographs and tests like anorectal manometry.
Are there other methods of IBS diagnosis?
Yes, the Manning criteria and another rarely used criteria called “Kruis.”
The manning criteria include:
- Pain relieved with defecation
- More frequent stools at the onset of pain
- Looser stools at the onset of pain
- Visible abdominal distention
- Passage of mucus
- A sensation of incomplete evacuation.
The more criteria it presents, the more the likelihood of IBS.
But the Manning and the Kruis criteria didn’t perform well in diagnosing IBS (compared to the Rome criteria).
So Rome criteria are considered the cornerstone for the diagnosis of IBS.
Take-Home messages:
- No specific and reliable test is available for IBS diagnosis.
- “Rome criteria” is the most widely used criteria for IBS diagnosis. They are symptom-based criteria.
- Other criteria exist for IBS diagnoses, like the Manning criteria and the Kruis criteria, but they’re less accurate.
- Rome criteria are only to guide diagnosis. We (doctors) may find some patients not matching the Rome criteria and still need IBS treatments.
- The diagnosis of IBS is individualized for every patient by the doctor.
- This article is a guide to simplify how IBS is diagnosed; you must consult your doctor before the final diagnosis.
You can also read our in-depth guide on how to relief IBS pain fast (within one day).